DHS Releases 2026/27 Blue Book; RCPA Shares Divisional Analysis
Author
Emma Sharp
Date
February 20, 2026
Share
In advance of the House and Senate hearings, the Department of Human Services (DHS) has released their “Blue Book” detailing the Department’s appropriations for the proposed 2026/27 budget. The proposed DHS budget reaches a total of $67.2 billion, with $21.9 billion in state funding, $39.7 billion in federal funding, and $5.6 billion in other funds, making it the largest spend category in the proposed budget.
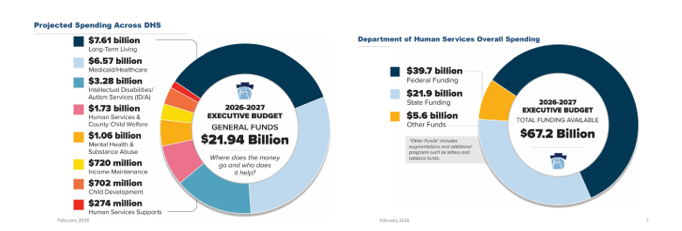
Within the DHS budget, Long-Term Living remains the largest expenditure of DHS’ state General Funds at approximately 35%, Medicaid healthcare delivery for both physical and behavioral health at 30%, and ID/A at 15%. The remaining 25% is spread across county child welfare, mental health and substance abuse, income maintenance, etc.
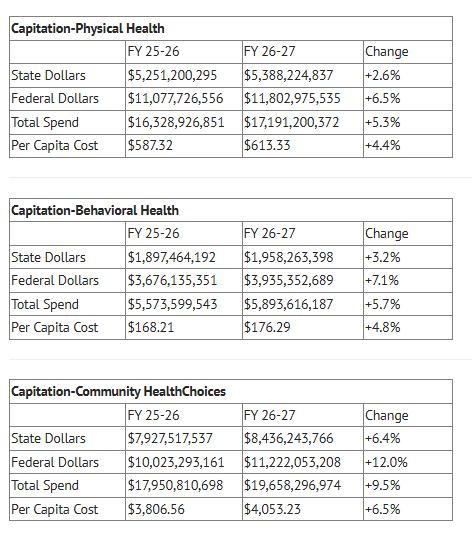
The Blue Book provides greater detail on the allocation of these funds, with particular detail regarding the Medicaid capitation and Fee-For-Service (FFS) appropriations. It also addresses Medicaid capitation rates. The budget proposal requests nearly $1 billion to reflect the changes in the number of eligible individuals and the rates paid by DHS to the MCOs due to higher acuity patients.
For FFS, appropriation shows that General Fund, QCA-funded, and Philadelphia Hospital Assessment payments are level-funded, which is consistent with FY 2025/26. These payments would include Inpatient, Outpatient, Medical Education, and Community Access funds, as well as QCA-solely funded payments, such as Rehabilitation, MA Dependency, Sole-Community hospital payments, and more. The FFS appropriation also reflects the proposed implementation of components of the Keystones of Health (1115 waiver). This includes services such as transitional housing, reentry supports, and food as medicine initiatives. Whether or not this is ultimately included relies upon the passage of the 1115 waiver, which is uncertain.
Key Highlights by Division:
Behavioral Health
- BH Capitation
The 2026/27 proposed budget includes a nearly 6 percent increase to $5.9 billion in behavioral health Medicaid capitation funding. Of this total, nearly $2 billion are state dollars, a 3 percent increase over the current fiscal year budget. The remainder are federal matching dollars. The behavioral health Medicaid capitation line item is the amount of money from which behavioral health Medicaid managed care organizations reimburse providers for mental health and SUD treatment services.
Intellectual and Developmental Disabilities
- Approximately 5.35% Increase for Community Waiver Programs: The budget proposes an approximate 2.8% increase in state funds over FY 2025/26 funding levels for the Intellectual Disability (ID) Community Waiver programs (Consolidated, Community Living, and PFD/S waivers). Corresponding increases in the federal funding shows an aggregate funding increase of 5.35% in this line item.
- It is important to note that this increase is not classified as a rate increase in any source documents.
- The funding appears primarily intended to carry forward existing services with recognition utilization trend cost increases.
- No Identified Rate Adjustments: The FY 2026/27 Blue Book materials do not reflect any proposed rate increases for ID community waiver programs.
- A lack of rate adjustments continues to raise concerns regarding system sustainability, including workforce stabilization and inflationary factors (e.g., wages, benefits, insurance, utilities).
- Providers should assume that the increase is not new discretionary funding but rather supports ongoing service costs.
- $30 Million for Partial-Year Funding of New Waiver Slots: The proposal includes $30 million in state funds to support:
- 400 new Consolidated Waiver slots; and
- 850 new Community Living Waiver slots.
IMPORTANT NOTE: The Blue Book citation indicates that this allocation provides six months of funding for these new slots. - Additional clarification is needed regarding whether this assumes a mid-year implementation (e.g., January 2027 effective date) or a phased-in enrollment process.
- Provider capacity (staffing, available beds, enrollment/licensing, etc.) will directly impact successful implementation of these additional slots.
- $2.9 Million for Annualization of Performance-Based Contracting (PBC) Initiatives: The budget proposes an additional $2.9 million in state funds to annualize previously implemented PBC initiatives.
- This appears to support the ongoing cost of PBC structures already put into place that were previously utilizing ARPA funding.
- The proposal does not include new, dedicated funding for future PBC expansions or additional administrative burden placed on providers.
- Ongoing ICF-to-Community Waiver Conversions: The budget indicates ongoing efforts to convert Intermediate Care Facility (ICF) beds into Community Waiver Programs.
- This continues previous efforts to move away from ICF programs to more integrated community-based services.
- ARPA Funding: ARPA funding provided under the American Rescue Plan Act of 2021 will be exhausted by June 30, 2026 per legislative requirements.
OLTL and Community HealthChoices
- The Community HealthChoices 2026/27 budget request continues to move the programs away from Fee-For-Service to Managed Care. The OBRA Waiver funding was reduced by an additional $50 million to less than $500 million in total. Meanwhile Community HealthChoices increased from $18.1 to $19.9 billion, an increase of 9.9%.
- The increase in Community HealthChoices reflects increasing levels of acuity of the participants served and an increase of approximately 1,000 new participants per month. No rate increases are projected in this budget. The increase in acuity was addressed through $212 PMPM in the MCO capitation rate.
- The only major opportunity for providers is in $87 million allocated to MCO Pay-For-Performance, which contractually includes targets for nursing home transition, improvements in HEDIS measures, and higher utilization of employment services.
Early Intervention
- After a record-setting 7% increase in Early Intervention Part C provider rates for 2025/26, a positive step towards narrowing the nearly 40% funding gap identified by the OCDEL rate study, the 2026/27 Blue Book shows a nearly 3.9% decrease in total funding for Early Intervention Part C. OCDEL leadership explains this decrease as apparent, not actual, and is due to the use of carryover funds from the prior year. This raises questions regarding these excess funds and any services that may have gone undelivered.
- The Blue Book also projects a decrease in Federal Medicaid dollars funneling through the EI program. This validates RCPA’s efforts, in conjunction with other stakeholders, to develop a pattern of long-term stabilizing funding increases in line with the OCDEL Rate Methodology Funding report and increase awareness and education campaigns focused on increasing actualization of all eligible Federal Medicaid funding for the program.
Contact your RCPA Policy Director with any questions.


